Recycling with the Humphrey ADE-circle system at very low fresh gas flows
Introducing myself
I am Dr David Humphrey, a medical anaesthetist involved in both medical and veterinary research since 1978. The Humphrey ADE-circle system includes a unique self-regulating 4-phase exhaust valve and, with other design changes, confers significant advantage over all other recycling systems. I use very accurate monitoring equipment and have published many papers, my results being verified independently in Medical and Veterinary anaesthetic journals. What I recommend below is based on thousands of observations. The Humphrey ADE-circle was first used in NHS hospitals in 1984, including Great Ormond Street Children’s Hospital, London. In 2000 vets started using it, and is now described in BSAVA manuals. In 2016 the RCVS recognized it as a simple, safe multi-purpose system; for their inspections no other system was needed.
Basic concepts: Why recycle?
With systems such as the T-piece, Lack, Mini-Lack, and Bain, the anaesthetic goes straight to the patient from where, on breathing out, it is all eliminated to atmosphere; all are simple “semi-closed” systems. Unfortunately, the significant penalty is that these semi-closed systems require much higher fresh gas flows (FGF) by as much as 7-8 fold when compared to recycling systems. Such high flows are cold, dry and cause hypothermia, while expired anaesthetic gases are hazardous to staff, polluting and cause ozone depletion, and are costly. Such detrimental consequences are no longer acceptable.
By contrast, recycling reduces fresh gas flow as much as 6-7 fold or more. This low flow is environmentally safer by reducing theatre and atmospheric pollution. The patient also gets a better anaesthetic because recycled gases are also warm and moist. Costs can be cut by sevenfold or more. It’s a WIN-WIN for everyone.
Some practices don’t recycle or use much higher FGFs than necessary, often around 2 l/min. What concerns staff is that recycling is not so simple and that they might make a mistake. The technique is different but there are some very simple rules to follow to give good, safe, low-flow anaesthesia. This is achieved with the multipurpose Humphrey ADE-circle system, a system significantly different in design from all other systems.
Recycling with the ADE-circle system; basic information
In a nutshell, the ADE system is used as a semi-closed system with a 500 ml reservoir bag for all small animals under 7kg without the soda lime canister. For all animals over 7kg, the canister is attached with a larger 1 or 2 litre bag. In both modes the FGF fresh gas flow set at 300-500 ml/min for all patients under 50kg. This will include most animals seen in small animal practise. For animals over 50kg flows increase by 10 ml/kg/min eg 80 kg dog requires 800 ml/min. I have anaesthetized a 260kg lion which required 2.6 l/min. Conclusion: It could not be simpler.
The only matter that requires attention when recycling at very low flows is ensuring the patient gets enough anaesthetic vapour to the brain. This is because the patient’s tissues absorb vapour and remove it from blood resulting in less vapour going to the brain. In practice, when using isoflurane, all that is needed is to add more vapour to the little fresh gas that is added to the system. My simple guideline is to use 3% instead of 1.5% isoflurane, 3.5% instead of 2% and adjust as necessary on clinical assessment. It’s simple, safe and it works. Even easier to use is sevoflurane which is magic; as it is minimally absorbed into the tissues, rarely is any adjustment necessary, while the stability of anaesthesia is remarkable. At such low flows, the cost of sevoflurane is dramatically reduced from over £13/hr to just £2/min at 300 ml/min – a saving of £11/hr!
Below is a more detailed but very useful guide to the ADE recycling technique. Please read it.
In more detail: What happens to carbon dioxide, oxygen and vapour when recycling?
The basic concept to understanding what happens within a recycling system with regards to vapour and oxygen concentration is illustrated in Fig 1 below. In essence the following sequence occurs when using isoflurane:-
- the patient removes oxygen and vapour (isoflurane) from the gas they breathe in.
- The oxygen and isoflurane content of expired gas is therefore less than they breath in. Both must be put back into the system when recycling.
- Expired gas is recycled through soda lime to remove carbon dioxide.
- The FGF at 10 ml/kg/min supplies double the oxygen uptake by the patient. It is therefore safe!
- The reduced isoflurane vapour in recycled expired gas dilutes the fresh gas – so much so that the patient may become light. This surprizes staff but very easily resolved
- The isoflurane replacement needs to be increased above normal % dialled settings.
- This requires turning up the vaporizer by 1-2% or more – but keeping the gas flow the same.
- This small increase in vaporizer setting might not seem cost-saving, but the fresh gas flow (FGF) at 300 ml/min is nearly 7 times less than average 2 l/minute used with other recycling systems.
- With sevoflurane, this adjustment is rarely necessary as almost no vapour is removed by the patient.
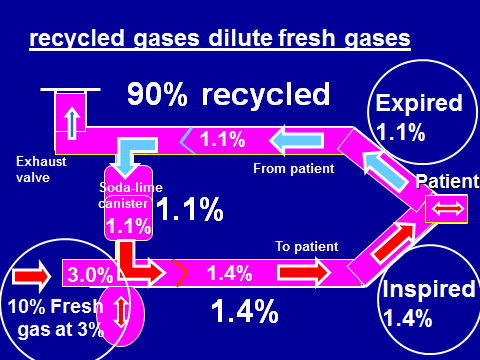
Fig 1 The diagram above illustrates the dilution effect of fresh gas by expired gas during low flow recycling through soda lime. The FGF of only 10% of the patient’s requirements is supplied into the system with the vapour set on the vaporizer at 3%. This 10% fresh gas at 3% isoflurane mixes with recycled expired gas at 1.1% isoflurane, being the other 90% of the patient’s fresh gas needs. The resulting mixture that reaches the patient may now fall to 1.4% – and not 3% as set on the vaporizer. This is almost half the vaporizer setting, but is not unexpected. To compensate, higher vaporizer settings of 1-1.5% are generally required to keep inspired gas vapour concentrations high enough to maintain anaesthesia, particularly with larger fat animals where more anaesthetic vapour is absorbed by tissues.
How to use the ADE-circle when recycling
Before recycling you must do a Leak Test: Before any attempt is made to recycle, the system MUST BE LEAK PROOF (instructions on the back of the Fresh Gas Flow Chart). Even if small, a leak may cause considerable problems in keeping the patient anaesthetized – usually too light. Hence it is absolutely essential that the system with the canister attached must be leak tested before every anaesthetic. It is surprizing how often this essential but simple pre-operative test isn’t done; it is so easy to do and takes a 20-30 seconds.
Removing carbon dioxide: This is easy to understand as carbon dioxide reacts chemically with soda lime and is removed from the anaesthetic gas. Soda lime turns a different colour when exhausted, so it is a condition that this must be checked and replaced as necessary (see the back of the Fresh Gas Chart that comes with the ADE-circle system (www.anaequip.com/fgf_chart). Soda lime in the canister lasts for variable periods. Large animals produce more carbon dioxide than smaller ones while more carbon dioxide will be removed when recycling at very low fresh gas flows. Both use the soda lime more quickly. As soda lime is inexpensive, it is best to change the soda lime monthly if not already indicated and to label the canister with refill date.
Replacing oxygen: Replacing oxygen is not a problem as the amount required is small – only around 5 ml/kg/min. For a 30 kg Labrador dog, the oxygen requirements would be just 150 ml/min. This miniscule flow really is all that is needed and would keep the reservoir bag full. However, such a low FGF would scare almost all vet anaesthetists! To add a 100% safety factor and also compensate for potential small leaks in the system or around the endotracheal tube, a minimum flow of 10 ml/kg/min is recommended, with a minimum of 300 ml/min (all animals under 30 kg the FGF is set at 300 ml/min). This FGF, although very low, is double what is required and is the recommended flow (as shown on the Fresh Gas Flow instruction sheet included with the ADE-circle system). This flow is therefore safe! However, see below for nitrous oxide use as higher combined flows of oxygen and nitrous oxide are required.
Nitrous oxide use when recycling: Although useful for its mild analgesic properties, this gas has been phased out of human anaesthesia as it is a hypoxic gas and its use can be hazardous. The same applies to veterinary use and, as in medical practice, the analgesic effect can be substituted by good analgesia in the pre-medication. Never-the-less nitrous oxide is useful.
When using nitrous oxide without the soda lime canister, the patient gets what is set. Normal settings for nitrous oxide/oxygen ratio is 2/1. At the minimum fresh gas flow of 300 ml/min, the setting would be 200 ml/min of nitrous oxide and 100 ml/min of oxygen.
However when recycling using the soda lime canister, the same nitrous oxide/oxygen ratio needs to be 50/50 ratio. The oxygen in the alveoli gets taken up and used by the patient while nitrous oxide remains much the same. Oxygen levels fall and, to avoid the potential for hypoxia, oxygen flow is always set at 50% of the mixture with nitrous oxide. The second condition is that the minimum oxygen supply must be 300 ml/min.
In practice the minimum flow is therefore be 600 ml/min, made up of 300 ml/min oxygen and 300 ml/min nitrous oxide. According to the Fresh Gas Flow chart, this is the maintenance flow for a 60 kg animal. As this FGF of 600 ml/min is the minimum fresh gas flow when using a 50/50 mixture of oxygen and nitrous oxide, this maintenance flow of 600 ml/min is set for all animals from 7-60kg.
Vapour concentration in semi-closed and recycling modes:
Important factors concerning anaesthetic vapour uptake and replacement need to be understood as knowledge inspires confidence and safety. Because recycled expired gas contains less vapour of unknown concentration, vapour concentration changes are inevitable especially at the much lower flows of just 300-500ml/min used with the ADE-circle. However, even though unknown, simple solutions get over this problem.
Semi-closed systems: When using the ADE system in the semi-closed mode (for small animals under 7kg), it is easy to understand what the patient is breathing. With the soda lime canister removed, there is no recycling; the FGF goes straight to the patient. The patient gets what you set on the vaporizer dial; you set 2%, the patient gets 2%. In this mode, the fresh gas flow is calculated at 70 ml/kg/min, very much lower than 300-500ml/kg/min with the T-piece (www.anaequip.com/veterinary_use for full details on why it is so efficient).
Recycling through soda lime: In contrast, when recycling through soda lime, the fresh gas flow is reduced to just 10 ml/kg/min – seven times less than in the semi-closed mode! With reference to Fig 1 above, almost all expired gas is recycled, usually over 90%! Isoflurane in expired gas has been removed by the patient as vapour is absorbed into the tissues while a little is metabolized by the liver. Consequently, vapour in expired gas is always less than that inspired – and it is this expired gas that is recycled. After passing through the canister where carbon dioxide has been removed, recycled gas with a lower vapour concentration now mixes with and dilutes with the fresh gas with a higher vapour concentration. The vapour dynamics are therefore potentially more complicated, but it is simple to correct any under-delivery of vapour to the patient by turning up the vaporizer by 1 to 1.5% and adjusting as required. However, with sevoflurane, this adjustment is rarely necessary as almost no vapour is removed by the patient.
Induction to wake up: Safe low-flow anaesthesia when recycling with the ADE system
Induction period: Initially on connection of the patient to the ADE-circle system, there is no anaesthetic gas in the system. The volume in the system is about 3 litres and this air needs to be washed out with 6 litres of anaesthetic gas. Once connected to the patient with the endotracheal tube sealed and leak proof, set the fresh gas flow is set at 3l/min for 2 minutes (total 6 litres), with the vaporizer set at about 50% higher than that used for maintenance eg 3% with isoflurane rather than 1,5%, and with sevoflurane 3.5% rather than 2.0-2.5%. After two minutes, reduce the flow to “induction” flows but keep the vaporizer at the higher setting. Remember that in this phase the patient is taking up a lot of isoflurane into the body tissues, and unless more vapour is added to the system during the induction period, the patient becomes lighter and may wake up as the IV induction agent wears off!
Maintenance period: On reaching surgical levels of anaesthesia after ±5 mins with isoflurane and only ±3 minutes with sevoflurane (longer with large and obese animals), the FGF can be reduced to maintenance flows but keeping the higher vaporizer settings. For all patients of 30kg or less this is only 300 ml/min. The higher vaporizer settings are still required as, with very low FGF, very little vapour is now being added to the system which must match the patient’s uptake – if too little they may become light. Once again, with sevoflurane this adjustment is rarely necessary as almost no vapour is removed by the patient. Should the patient require a rapid increase in the depth of anaesthesia. only then for a quick increase in vapour concentration should the flow be increased for a minute or two as well as increasing the dialled vapour %. Towards the end of anaesthesia, gradually turn down the vaporizer, and when complete, turn it off, squeeze the reservoir bag and increase the oxygen to 3-4 l/min to wash out any anaesthetic from the system.
In summary, the expired gas always dilutes the vapour in the fresh gas being added to the system. With the very low fresh gas flows used with the ADE system, most of the expired gas (over 90%) is recycled gas so this dilution effect is significant. The good news is that it is easy to compensate for this effect. All you have to do is add more vapour to the fresh gas by turning up the vaporizer by 1-1.5%, keeping the fresh gas flow at recommended levels. As an anaesthetist and use an agent monitor on all patients, I generally find that inspired isoflurane level is about half the dialled concentration which I find is a useful guide. I’m therefore not scared to set 3.5% isoflurane knowing that patient is getting about 2%. But be aware that large fat animals soak up vapour – and hence a lot of vapour needs to be added back. It is these patients who often become light if the dialled % is not increased to the levels I recommend above. With sevoflurane almost all the problems described above are minimized as it is minimally absorbed into tissues. Almost all that goes in comes out; even at the low flows, sevoflurane is an incredibly stable anaesthetic agent.
Cost savings: It is obvious that if the fresh gas flow when recycling uses 7 times less, then costs of both vapour and oxygen will be reduced by the same amount. With sevoflurane at £13/hr at 2 l/min, the ADE-circle reduces this cost to £2/hr at 300 ml/min – saving £11 per hour! See the savings chart of the website www.anaequip.com/ade/.
It may seem that costs are increased if the vaporizer is set higher as recommended above, but at such low flows you will still save a lot of money and reduce pollution. Using a low FGF of 300 ml/min at 3% isoflurane still costs over 4 times less than 2% at 2 l/min commonly used with other circle systems (eg “the hamster wheel”). In addition, the animal gets a better anaesthetic as expired gas is warmed and humidified – the necessity for body warmers is reduced! An activated charcoal absorber will also last much longer as little is directed to it.
Conclusion: It is easy to control anaesthetic depth when recycling. At very low flows vaporizers settings with isoflurane need to be increased by 1-1.5%. With sevoflurane these adjustments are not usually required.
Warning:
The FGFs recommended above only apply to the Humphrey ADE-circle system and not to other circle systems. The new ADE self-regulating 4-phase exhaust valve and other design changes confer significant advantage over all other recycling systems such the round “hamster wheel” or “U” canisters. These canisters are poorly designed because they save expired gas but waste fresh gas. It is these older canister designs that require higher fresh gas flows. Conversely and more logically, the Humphrey ADE-circle systems saves fresh gas and eliminates alveolar gas!